When we have medical problems, we all want to understand the ‘who’, ‘how’ and ‘why’ of the condition. Knowing may lead to changes or corrections that might fix and potentially remove the problem. Many professionals have invested their careers studying obstructive sleep apnea (OSA), trying to understand the ‘hows’ and ‘whys’ of OSA. It remains a subject that few professionals agree upon. Perhaps it’s best to review the broad landscape of OSA before we look at the details; reviewing the forest before the trees. Let’s look at the ‘who’ of OSA.
OSA is a common condition. How many people have it and what are their characteristics? We have a general outline for the answers to these questions and it is best to start with an understanding of those facts. First, how common is it?
Investigators have studied and reported answers to our questions, but the answers seem to change with each report. There are real reasons for the differing answers. Depending upon the how the information was obtained, the answers will vary. The source of the estimates can be from formal research designed to uncover the answer, population studies of many types, questionnaire reviews, insurance data reviews, or combinations of these and other techniques. The frequencies reported range from highs of 50% from Germany and 37% from Switzerland, to lows of 3% in Australia. When reviewing these reports, one is struck by the differences in how people were selected for inclusion in the studies; the variations in the definitions used to label someone as having OSA and by the increasing level of its reported occurrence as the years passed and the condition became more commonly known.
The differences in these reports are not hard to understand. Each has a specific method to gather potential individuals into the report. Enrollment into the study varies. In many reports, the individuals have to volunteer to provide private medical information. Even the report from closed medical populations in countries with government run medical systems cannot identify cases if the individuals do not participate. The wise blind man can only grasp what he can feel and the wise investigator can only see what he has chosen to look at.
Another factor to take into account is how the report defines ‘having OSA’. Are test results required? If so, what kind of test and what parameters are necessary to establish the diagnosis? What level of OSA does the study accept? Does it include what is generally considered to be mild OSA (5-15 apnea event per hour)? Does it require the higher level of moderate OSA (greater than 15 event per hour) or does it include both and how are they reported? Each report varies.
Many details chosen by investigators will determine the population they report and thus, the prevalence of the condition. Reviewing for this presentation, I went to the National Library of Medicine website to look for appropriate information. My search identified 10,388 articles with information about the prevalence of obstructive sleep apnea.
Prevalence is the frequency of occurrence of something (in this case obstructive sleep apnea) in a selected defined population.
The important fact is that this condition is very common. How common is it? No consensus exists. The table below is constructed from several studies over the last 30 years and gives you an idea of reported values and how they have increased over the years.
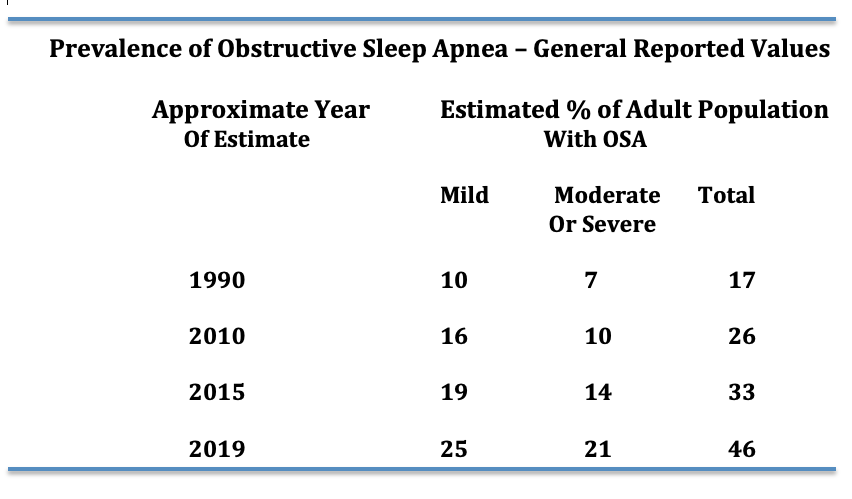
I believe it is safe to say that at least 20 to 25% of adults in the United States have mild or greater apnea. Why the increase in prevalence with passing years? It is unclear, but most likely it represents the increase in awareness of the problem.
But, we need to be aware of still more details about who experiences OSA
Age is an important factor when measuring the prevalence of OSA. Few reports have elderly individuals participating. However, the report from Germany on 4,420 individuals from 20-81 years provides some answers. Half of the population had at least mild OSA and 20% had moderate or severe OSA. When broken down by age, 80% of men 70 y/o and older had some degree of OSA. The Swiss study also demonstrated a significant increase with age. Older studies do not show such a high prevalence in the elderly, but the majority of them did not include elderly individuals in the populations studied. Time will tell, but obstructive sleep apnea is very common in the elderly.
There is evidence that some ethnic groups may have more Obstructive Sleep Apnea than others. Particularly individuals of Southeast Asian or Black heritage. It is proposed that the cranial and facial boney structure in those groups leads to smaller upper airways.
What about occurrences during our youth and young adulthood? OSA is known to occur in infancy, childhood and during the teenage years. The prevalence for those ages is considered to be between 1 and 5%. As for early adulthood, there is substantial information from multiple reports to indicate it occurs in 5% to 8% of 18-30 year olds.
In the summary above I have used numbers that include both sexes. There is a significant difference in the occurrence of OSA between the sexes. In the report from Switzerland, 50% of men and 24% of women in the report had OSA. For most reports a significant difference between men and women is noted during the premenopausal years. With aging and menopause, the occurrence of OSA in women increases.
Summary – The Prevalence of Obstructive Sleep Apnea
The frequency increases with age in both sexes. After the age of 70, the occurrence rate is dramatic reaching up to 80% of adults in one study.
It is more common in men than women. After menopause the occurrence in females increases significantly
References:
Prevalence and association analysis of obstructive sleep apnea with gender and age differences. Fietze et al. J Sleep Res 2019 Oct; 28(5):e12770
Estimation of the global prevalence and burden of obstructive sleep apnea: a literature-based analysis. Benjafield et al. Lancet Respir Med. 2019Aug; 7(8):687-698
Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. R Henzer et al. Lancet Respir Med. 2015 Apr; 3(4): 310-318
Screening for Obstructive Sleep Apnea in Adults US Preventive Services Task Force Recommendation Statement. JAMA January 24/31 2017; 317(4) 407-414
Diagnosis and management of childhood obstructive sleep apnea syndrome. Marcus CL, Brooks LJ, Draper KA, Gozal D, Halbower AC, Jones J, Schechter MS, Ward SD, Sheldon SH, Shiffman RN, Lehmann C, Spruyt K, American Academy of Pediatrics. Pediatrics. 2012;130(3):e714.
RGH